A Delayed Presentation of Congenital Diaphragmatic Hernia
A report describes a case of a 17-year-old female with a history of anxiety who presented with an 18-hour history of intense left upper quadrant (LUQ) abdominal pain that worsened with movement. She denied any recent abdominal trauma or dietary changes but reported experiencing similar episodes of pain twice, with the last episode two years ago. Her laboratory investigations, abdominal ultrasound, and pregnancy test were normal, and on the improvement of pain, she was discharged home.
One month later, the patient returned with similar LUQ abdominal pain, VAS for pain as 7/10, and limited ambulation. She also documented chest tightness while lying flat, nausea, and an episode of nonbloody, nonbilious emesis.
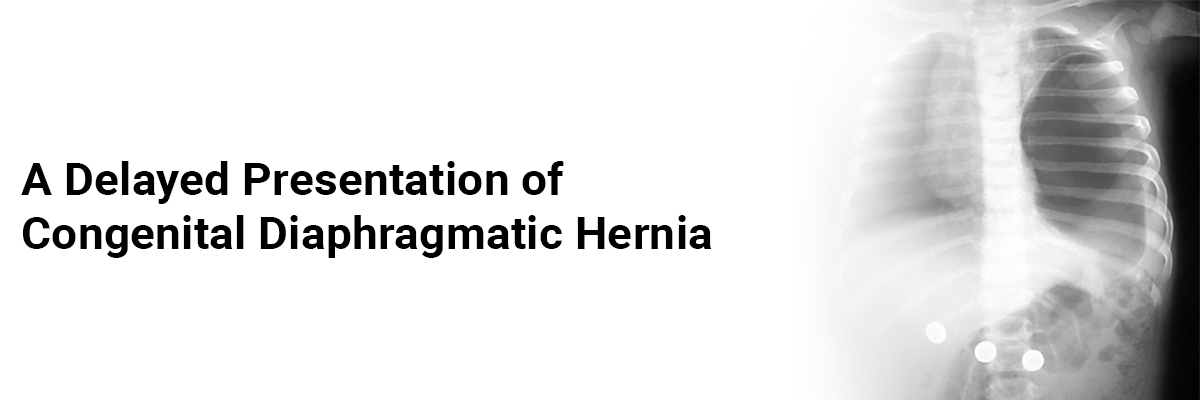
The patient's vital signs, complete blood count, urinalysis, complete metabolic panel, and lipase came normal, while an abdominal CT scan showed a left hemidiaphragm defect with a colon above the left diaphragm. (which were not seen on her recent abdominal ultrasound and a chest radiograph obtained 14 years before). The diagnosis of congenital diaphragmatic hernia (CDH) was made and was scheduled for surgical repair in one month. However, two days later, the patient experienced severe LUQ abdominal pain that caused a syncopal episode. She received a combination of acetaminophen, ibuprofen, gabapentin, and oxycodone, which improved her pain. On discharge, the patient minimized physical exertion and adhered to a pain control and bowel regimen. One month later, she showed a successful laparoscopic diaphragmatic repair and remained symptom-free for over a year.
Vinton V, Posa M, Kelly MN, et al. Beyond the Neonate: A Delayed Presentation of Congenital Diaphragmatic Hernia in a 17-Year-Old. Case Rep Pediatr. 2024 May 15;2024:7518183. Doi: 10.1155/2024/7518183.

Recent FAQs





Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article