A rare case of Weil’s disease (leptospirosis) in pregnancy
A 23-year-old primigravida, at 34 weeks of gestation––with a vertex presentation and Rh-negative status––was transferred from a peripheral hospital to our tertiary care center due to severe bradycardia and hypotension. She reported reduced fetal movements but was not in labor.
Her medical history included bilateral lower limb swelling for 15 days, cough with expectoration, sore throat, dysphagia for eight days, and epistaxis a week prior. Additionally, she experienced fever, jaundice, dark-colored urine, and hematochezia over the past four days.
She had no known history of pregnancy-induced hypertension (PIH), gestational diabetes mellitus (GDM), or cardiac, renal, or thyroid disorders.
On examination, the mother was conscious and oriented but febrile at 100°F, with severe icterus, bilateral grade 3 pedal edema, and a toad-skin appearance. Her pulse was feeble at 46 bpm, with a blood pressure of 80/50 mmHg in both upper limbs. The uterus measured 32 weeks in size and was relaxed, with the fetal head in the lower pole and fetal bradycardia at 90-95 bpm.
Given the severity of her condition, ICU admission and pregnancy termination were discussed with her family. She was started on intravenous noradrenaline, and blood samples were collected for laboratory evaluation.
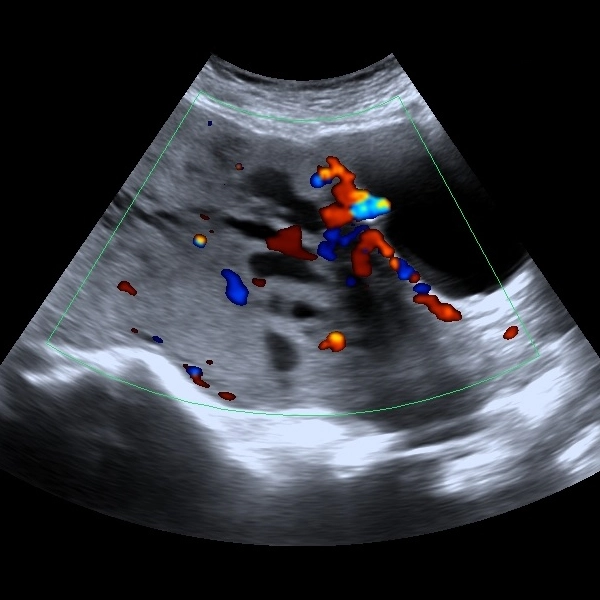
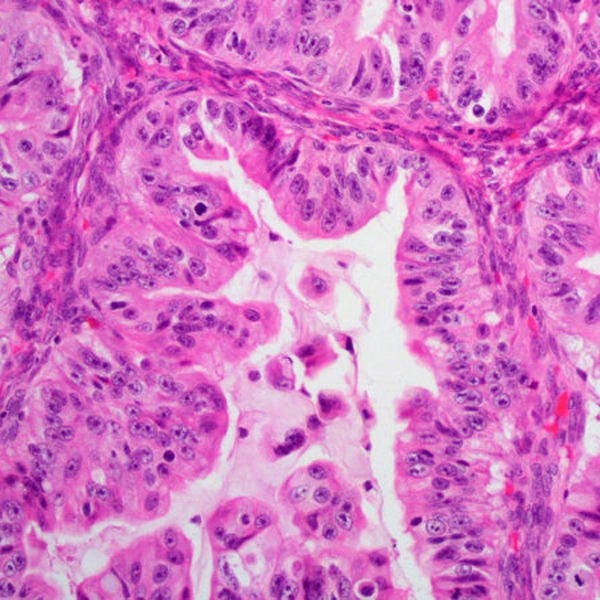
Investigations revealed anemia (Hb: 6.1 g/dL), acute kidney injury (creatinine: 2.2 mg/dL), hyperbilirubinemia (total: 9.7 mg/dL, direct: 8.5 mg/dL), and coagulopathy with prolonged aPTT (>120 sec). Serological testing confirmed leptospirosis (IgM positive). Ultrasonography (USG) showed grade 1 fatty liver and intrauterine fetal demise. A Foley catheter was inserted, and she received intravenous piperacillin (4.5 g every 12 hours), vitamin K (10 mg), and oral ursodeoxycholic acid (300 mg twice daily). Due to severe coagulopathy, she was transfused with packed red blood cells (PRBCs), fresh frozen plasma (FFP), cryoprecipitate, and platelets.
Labor was induced with a Foley catheter and oxytocin infusion. However, 24 hours post-admission, she developed hematemesis, hemoptysis, and epistaxis with labor arrest. Repeat investigations showed worsening coagulopathy and thrombocytopenia, necessitating additional blood product transfusions.
Due to failed induction and maternal distress, an emergency lower-segment cesarean section (LSCS) was performed, delivering a stillborn male weighing 2.4 kg. Postoperatively, she developed severe postpartum hemorrhage, unresponsive to medical management, requiring stepwise devascularization and peripartum hysterectomy. After achieving hemostasis, an intraperitoneal drain was placed, and she was transferred to the ICU.
On postoperative day 2, she exhibited persistent hypotension, reduced urine output, and ascites, with a 24-hour drain output of 1100 mL. Her hematological, hepatic, and renal parameters continued to deteriorate despite aggressive resuscitation, including transfusion of PRBCs, FFP, and platelets. Despite intensive care, she succumbed 24 hours after surgery.
Leptospirosis awareness, preventive measures - direct or indirect contact avoidance with animal urine, and the implementation of rodent control, are crucial. Due to symptom overlap, leptospirosis should be considered in the differential diagnosis of viral hepatitis and obstetric cholestasis. Additionally, in late pregnancy, jaundice, hemolysis, elevated transaminases, and coagulopathy necessitate differentiation from HELLP syndrome and acute fatty liver of pregnancy (AFLP).
Source: Ginjupalli A, Movva N, Owk R, Gowda R. J OBGYN. 2024;10(2):446-9.



Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article