Case Report of Paraganglioma Associated with Hypertension During Pregnancy
A 25-year-old pregnant woman––at 31 weeks gestation––was admitted after a hypertensive episode during a dental procedure.
Previously healthy, she had a pregestational BMI of 18 kg/m².
On admission, she was detected with a supine BP of 150/90 mmHg and HR of 130 bpm. No lower limb edema was noted.
Blood analysis revealed mild anemia and leukocytosis without deviation and altered inflammatory tests – leading to a presumptive diagnosis of preeclampsia. Her BP was uncontrolled control, which was followed by hyperglycemia emergence. Further history revealed palpitations and sweating – persisting throughout her gestation.
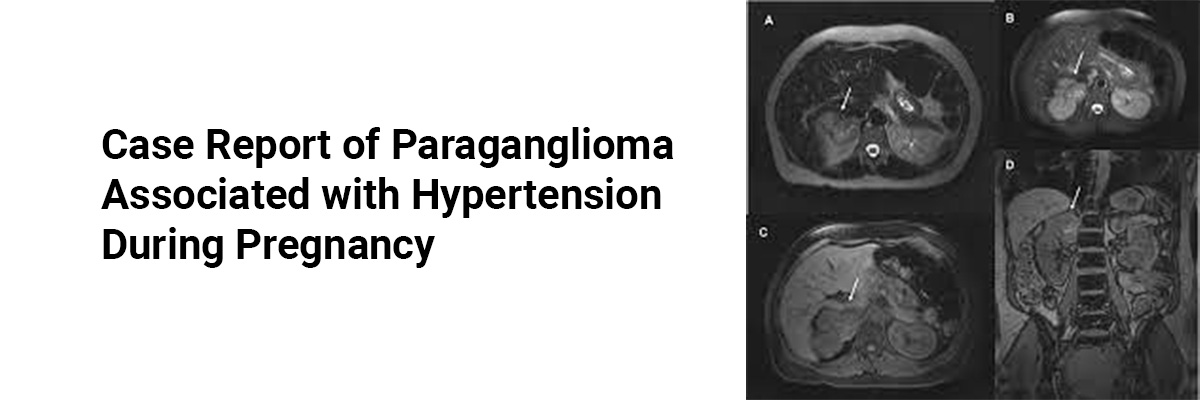
MRI revealed a 41 × 33 × 42 mm retroperitoneal mass near the right kidney. Plasma metanephrines were elevated, confirming the suspicion of Paraganglioma (PPGL).
Due to the unstable HT, an emergency cesarean section was performed at 32 weeks gestation without prior adrenergic blockade. During surgery, her BP spiked to 260/192 mmHg, and HR reached 225 bpm. Postoperatively, the patient was treated with norepinephrine and sodium nitroprusside, followed by oral alpha-blockers, which contraindicated breastfeeding. The newborn weighed 2370 grams and had Apgar scores of 8 and 9 at 1 and 5 minutes.
Plasma normetanephrines remained elevated post-delivery, and scintigraphy confirmed the PPGL. A video-laparoscopic mass resection was performed four months later after a successful adrenergic blockade, and pathology revealed a 19 g PPGL.
Postoperatively, BP and glucose levels normalized, and the patient experienced no complications.
PPGL should be considered in pregnant women with early-onset HT, as inappropriate diagnosis can lead to severe maternal and fetal complications. Genetic counseling is recommended in such cases––during the reproductive age.
Source: Giorgi RB, Aroucha PT, Favreto TM, et al. Case Rep Obstet Gynecol. 2024;2024:6655229.

Recent FAQs





Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article