Fatal Coronary Artery Anomaly in a Young Athlete Presenting as Syncope
A 14-year-old boy was brought to the emergency department after experiencing syncope and afebrile seizures. Three days earlier, he collapsed during a soccer game and had generalized tonic seizures with median ocular fixation. The seizures resolved spontaneously after about 10 minutes without the need for cardiopulmonary resuscitation. When the ambulance arrived, he was nearly alert, with stable vital signs, and was taken to a nearby hospital. There, a physical examination showed no signs of trauma, dehydration, or abnormalities in the respiratory, circulatory, or neurological systems. An electrocardiogram revealed no arrhythmias or ST-T abnormalities, and head MRI and general blood tests, including cardiac enzyme measurements, were normal. He was observed in the hospital and discharged the next day. Due to the limited ability of the initial hospital to perform a thorough cardiovascular examination and its distance from his home, he was referred.
His medical history included mild asthma and was negative for a known cardiac disease, arrhythmia, or a family history of sudden death.
On detailed history taking, the patient reported experiencing severe anterior chest pain followed by a blackout just before collapsing during the soccer game. He also mentioned brief episodes of chest discomfort during exercise in recent weeks.
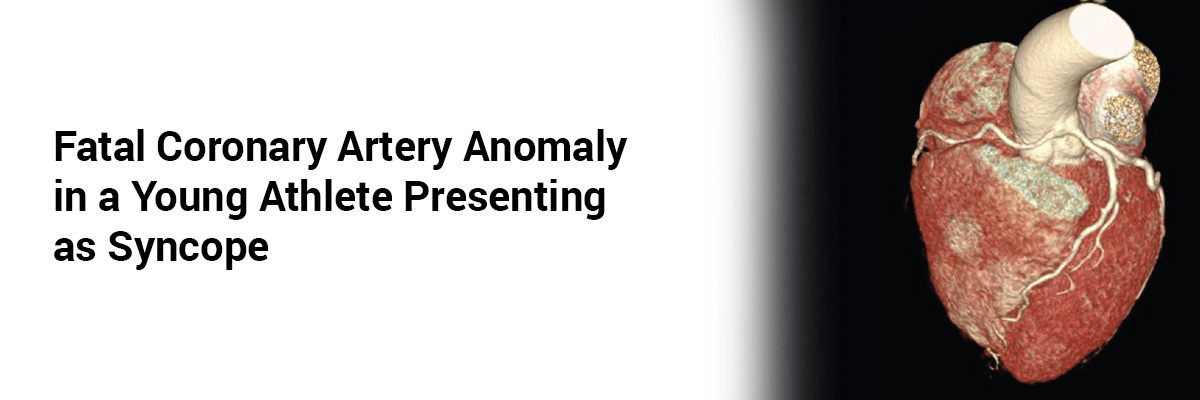
Suspecting cardiogenic syncope, we performed an echocardiogram, which showed the left coronary artery in its normal position. However, coronary computed tomography angiography (CCTA) revealed that the left coronary artery originated from the right sinus of Valsalva, with part of the left main trunk being intramural. The artery had an acute take-off angle from the aorta and a slit-like ostium. Electroencephalography results were normal. A treadmill exercise test (Bruce protocol) and myocardial scintigraphy (resting and exercise stress) achieved a target heart rate of 175 bpm without inducing chest symptoms, myocardial ischemia, or arrhythmia.
The patient was diagnosed with the anomalous aortic origin of the left coronary artery from the right sinus of Valsalva with an intramural course (AAOLCA-IM) and referred for early cardiac surgery due to the high risk associated with this condition and his desire to continue playing soccer. Exercise was restricted until surgery.
The operation involved unroofing the intramural segment and enlarging the new left coronary artery orifice with a patch using a great saphenous vein graft. The surgery was successful, and the patient was discharged two weeks later. He was prescribed aspirin for six months and gradually resumed physical activities. Follow-up visits showed he could play soccer without symptoms.
Symptomatic AAOLCA-IM poses the highest risk of sudden death among anomalous aortic origins of coronary arteries (AAOCA) and often necessitates surgical intervention. Cardiogenic syncope in children, though rare, can lead to serious cardiovascular events, including sudden death. Syncope during exercise or preceding chest pain is a critical indicator of cardiogenic syncope and should prompt cardiovascular imaging evaluation.
Source: Ifuku T, Nakatani K, Ueno K, et al. Case Reports in Pediatrics. 2024;2024(1):6390066.
Recent FAQs





Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article