Modified Lung Ultrasound Score: An Improved Approach for Early Detection of Acute Respiratory Distress Syndrome in Pediatric Patients
Lung ultrasound scoring is a proven tool for evaluating lung pathology. Despite the presence of scoring systems, the size of consolidations gets usually overlooked, which can reduce their accuracy in specific clinical situations.
This case study was conducted on an eight-month-old child admitted to the PICU due to severe pediatric acute respiratory distress syndrome (PARDS) caused by influenza A. The child arrived with respiratory failure requiring intubation, and extracorporeal life support (ECLS) was started on the first day of hospitalization due to critically low oxygen saturation (70-75%) and low blood pressure (mean below 40 mmHg), despite treatment with Noradrenaline, Dobutamine, and inhaled nitric oxide. Initial blood gas analysis showed severe acidosis (pH 6.98) and high carbon dioxide levels (pCO2 120 mmHg).
Ventilation settings were adjusted to a positive end-expiratory pressure (PEEP) of 12 mbar and peak inspiratory pressure (PIP) of up to 50 mbar. Neck cannulation was performed to start veno-arterial extracorporeal membrane oxygenation (ECMO), followed by a lung rest strategy with reduced ventilation settings. On the second day, PEEP was increased to 8 mbar, and surfactant inhalation was implemented alongside regular repositioning of the patient. Over time, tidal volumes improved, leading to the discontinuation of ECLS on day 14, although mechanical ventilation continued until day 17. The patient was discharged after 27 days without complications.
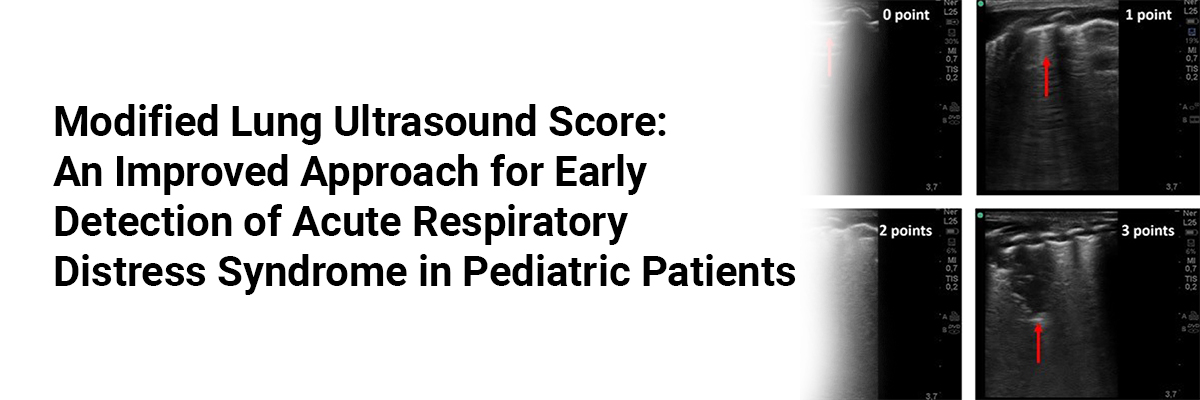
Additionally, the study evaluated modified lung ultrasound score (LUS+) daily through stored images, videos, and bedside assessments. Spearman’s correlation indicated strong agreement between modified and conventional LUS methods (R values ranging from 0.93 to 0.99). Improvements in LUS+ were noted starting on day 5, coinciding with the end of lung rest and correlated with enhancements in lung opacity, Brixia Score, and RALE Score. Additionally, conventional LUS and tidal volumes showed improvement beginning on day 9, with both modified and conventional LUS demonstrating similar results after day 12.
This study presents a modified LUS+ for bedside use, allowing assessment of stored images without additional technical support. It can quantify consolidation sizes, making it particularly useful for severe cases like large pneumonias and PARDS. Thus, incorporating consolidation depth measured in centimeters is a significant improvement to the conventional LUS, increasing its effectiveness in monitoring pediatric patients with acute respiratory distress who are receiving extracorporeal life support (ECLS).
Source: Küng E, Aichhorn L, Di Nardo M, Cardona F, Berger A, Milos RI, Watzenböck M, Brandt JB. Modified lung ultrasound score for improved monitoring of pARDS on ECMO, a case report. BMC Pediatr. 2025 Jan 16;25(1):36. doi: 10.1186/s12887-024-05308-7. PMID: 39819488; PMCID: PMC11736947.

Recent FAQs





Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article