 IJCP Editorial Team
IJCP Editorial Team
Mucormycosis of pouch of douglas in a diabetic lady: Report of a rare case
Abstract
Mucormycosis is a severe fungal infection which is rare in clinical practice. This infection is usually acquired by inhalation; other portals of entry are ingestion and traumatic implantation, especially in immuno-compromised patients. Here, we present a case of mucormycosis in a 44 year old diabetic woman. The patient had collection of fluid in the Pouch of Douglas and history of bleeding per vagina. Hysterectomy was done which showed a blackish serosal surface of the posterior uterus. Subsequent investigations revealed mycormycosis affecting the pouch of Douglas. Patient was treated with liposomal amphotericin B and is now keeping well.
Introduction
Mucormycosis, also known as zygomycosis or phycomycosis is an uncommon, opportunistic fungal infection caused by Mucorales of class Zygomycetes and usually affects immuno-compromised persons.1 Risk factors for acquiring this infection include uncontrolled diabetes mellitus, hematologic disorder, hematopoietic or solid organ stem cell transplantation, Surgery/trauma, burn wounds, corticosteroid therapy, autoimmune disorder and HIV infection. Mucormycosis is certainly less common than candidiasis or aspergillosis. But recent studies have shown an increase in the incidence of this infection in the United States of America and Europe.2 The rise may be due to better diagnostic facilities, increase in the incidence of diabetes mellitus and HIV infection; and also use of immunosuppressive drugs in modern therapeutics.
Case Report
A 44 year old woman presented with abdominal pain and fever for the last three months and irregular bleeding per vagina for three years. The lady was a known diabetic for 12 years. Routine examination revealed hemoglobin 9.1gm/dl, total white blood cell count 11,200/mm 3 with neutrophil 77%, lymphocyte 18%, eosinophil 4%, monocyte 1%. Platelet was adequate (2.7lacs/mm 3) Fasting blood sugar was 170mg/dl and post prandial blood sugar was 230mg/dl.
HbA1C was 9.7 on admission. Physical examination revealed pallor and rise in temperature. Chest was clear and liver and spleen were not palpable. Per vaginal examination revealed bulging and tender Pouch of Douglas. Ultrasonography (USG) showed fluid collection (30ml) in the Pouch of Douglas (POD), and thickened peritoneal covering over the posterior aspect of uterus. No organomegaly or other abnormality was found during whole abdominal USG examination. Colposcopic examination was done and fluid from POD was taken out for cytologic examination and to rule out malignancy.
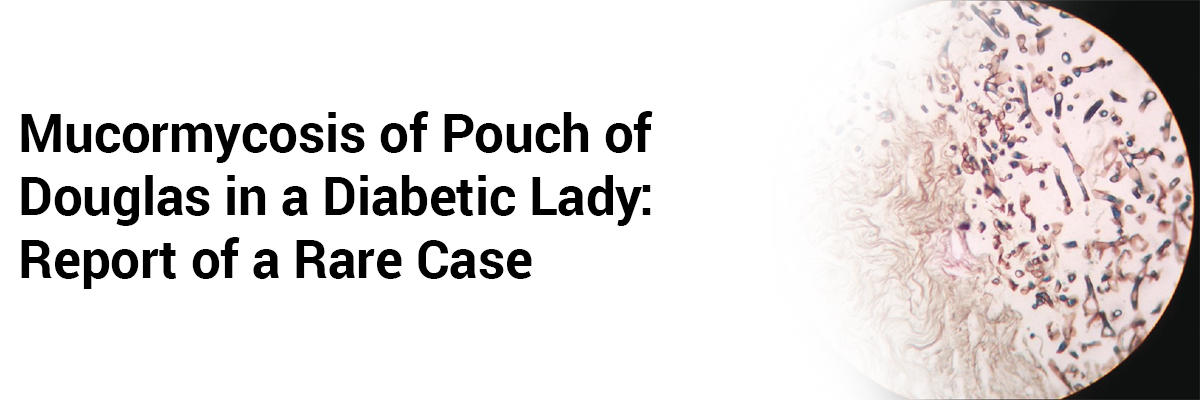
Cytologic smears revealed inflammatory cells with a predominance of lymphocytes. No malignant cell was detected. Broad spectrum antibiotics were given to the patient but of no avail. A decision of hysterectomy was taken as the patient was suffering from dysfunctionaluterine bleeding for a long time (three years) and her family was complete. Grossly, the uterus measured 9.5 × 6 × 4.5 cm. Posterior outer surface was blackish with variegated appearance. Tissue taken from that blackish area was sent for culture examination and remaining tissue was fixed in formalin and sent for histopathologic examination. Microscopical examination, revealed fungal elements in the myometrium and predominantly in the serosal layer in Hematoxylin and Eoisin stain. No granuloma was detected. Special stain like Methanamine silver stain (Grocott) was done which showed broad aseptate, right angle branching, ribbon like hyphae of Mucormycosis. Culture of the tissue in Sabouraud dextrose agar also showed growth of mucormycosis. Patient was given intravenous liposomal Amphotericin B and broad spectrum antibiotics. At the same time, she was given insulin to control diabetes. After treatment the patient recovered well and now is doing routine work.
Discussion
Mucorales, the infective agent causing Mucormycosis are present in soil, decaying material, bread, fruit, and usually non infective to normal human beings. They attack the immuno-compromised persons.3 Invasive mucormycosis is classified into six different clinical syndromes depending on the anatomic location of the disease. These are: rhino- cerebral, pulmonary, gastrointestinal, cutaneous, disseminated and miscellaneous.4 Rhinocerebral is the most common form, followed by pulmonary infection. Mucormicosis of the Pouch of Douglas is extremely rare and we did not find any such case in English Literature till date. Intact mucosa and endothelium in normal persons act as barrier to this infection and prevent tissue invasion and angioinvasion. Likewise mucormycosis is rarely seen in patients who have apparently normal skin. Primary cutaneous zygomycosis/mucormycosis is seen when skin is disrupted (like burns, soft tissue trauma, etc.) in immnocompromised persons and in premature neonates. Disseminated Mucormycosis has the worst prognosis and mortality rate approaches 100%.4 Mucormycosis can infect any part of the body and cases have been reported in parotid gland, ear, spinal cord, knee joint, urinary tract, genital organs and the pelvic floor.5 In our case though the patient was diabetic, how mucormycosis affected the Pouch of Douglas is still unanswered. Possible explanation might be instrumental trauma (during fluid collection laparoscopic/colposcopic) which predisposed the diabetic patient to acquire this infection. A high percentage (45%) of co infection with Aspergillus species has been reported.6 But in our case, no such co-infection has been found. Moreover, epithelioid granulomas in mucormycosis as reported by others were also absent in this case.4 In our case the patient had uncontrolled diabetes (Hb A 1 C 9.7, fasting sugar 170mg/dl and PP blood sugar 230mg/dl) which might be a risk factor to acquire this fungal infection. But a decreasing number of published mucormycosis since 1990 in patients with diabetes mellitus was reported by some authors. This might be due to better glycemic control and decreasing rates of diabetic ketoacidosis and widespread use of statins.7 However diabetes mellitus and hematologic disorder/malignancy remain major risk factors for mucormycosis.8 Diagnosis of mucormycosis is a challenging job as clinical manifestations are extremely variable. In the early stage, the infection is undiagnosed most of the time due to clinical non suspicion of this rare disease. Routine hematologic findings are non-specific such as leukocytosis, acidosis or hyperglycemia. Serological tests are of no use. Blood culture reports are usually negative though rarely fungal growth in the blood (fungaemia) has been reported. Obtaining tissue biopsy from the affected area is important to diagnose these cases. Special stains (silver stain, periodic acid Schiff) are used to confirm the fungal elements.
Medical textbooks and literature highlight three important aspects regarding treatment of mucormycosis. These are (1) reversal of risk factors/ underlying conditions. (2) medical therapy and (3) surgical debridement.10 Both conventional and liposomal Amphotericin B is effective against Mucor; but the liposomal form offers less infusion site side effects and less nephrotoxicity. The duration of therapy varies from weeks to months.[9],[10] In our case the patient was given liposomal amphotericin B 1mg/kg/day for one month along with a broadspectrum antibiotic Meropenem 1gm q 8h. Invasive mucormycosis is gaining more grounds and commonly seen in immunocompromised persons. Early tissue diagnosis along with culture is an important part of diagnostic work up. Adequate resection/ debridement of infected tissue and rapid initiation of a systemic antifungal therapy should be started immediately as mortality rate of this infection is very high.
About the Authors
Santosh Kumar Mondal, Palash Kumar Mandal, Tanmoy Kumar Mondal, Nandita Basu
Department of Pathology, Medical College, Kolkata, India
Department of Gynecology and Obstetrics, Burdwan Medical College, West Bengal, India
Department of Pathology, Medinipore Medical College, Medinipore, West Bengal, India
References
- Sugar AM. Agents of mucormycosis and related species. In: Mandell GL, Bennett GL, Bennett JE, Dolin R. Editiors. Mandell, Douglas and Bennett’s principles and practice of infectious diseases. 5 th ed. Philadelphia: Churchill Livingstone; 2000. p. 2685- 95.
- Lass-Florl C. The changing face of epidemiology of invasive fungal disease in Europe. Mycoses 2009;52:197-205.
- Lo OS, Law WL. Ileocolonic mucormycosis in adult immunocompromised patients: A surgeon’s perspective. World J Gastroenterol 2010;16:1165-70. [PUBMED]
- Waness A, Dawsari GA, Jahdali HA, The rise of an opprrtunistic intection called “Invasive Zygomycosis”. J Global Infect Dis 2009;1:131-8.
- Williams JC, Schned AR, Richardson JR, Heaney JA, Curtis MR, Rupp IP, et al. Fatal genitourinary mucormycosis in a patient with diagnosed diabetes. Clin Infect Dis 1995;21:682-4. [PUBMED]
- Sageman V, Maertens J, Meersseman W, Spriet I, Verbeken E, Lagrou K. Increasing incidence of mucormycosis in University Hospital, Belgium. Emerg Infect Dis 2010;16:1456-8.
- Kontoyiannis DP. Decrease in the number of reported cases of zygomycosis among patients with diabetes mellitus: A hypothesis. Clin Infect Dis 2007;44:1089-90. [PUBMED]
- Roden MM, Zaoutis TE, Buchanan WL, Knudson TA, Sarkisova TA, Schaufele, et al. Epidemiology and outcome of zygomycosis: A review of 929 reported cases. Clin Infect Dis 2005;41:634-53.
- Konotoyiannis DP, Lewis RE. Invasive zygomycosis: Update on pathogenesis, clinical manifestations and management. Infect Dis Clin North Am 2006;20:581-607.
- Rogers TR. Treatment of zygomycosis: Current and new options. J Antimicrob Chemother 2008;61:35-40. [PUBMED]
IJCP Editorial Team
Comprising seasoned professionals and experts from the medical field, the IJCP editorial team is dedicated to delivering timely and accurate content and thriving to provide attention-grabbing information for the readers. What sets them apart are their diverse expertise, spanning academia, research, and clinical practice, and their dedication to upholding the highest standards of quality and integrity. With a wealth of experience and a commitment to excellence, the IJCP editorial team strives to provide valuable perspectives, the latest trends, and in-depth analyses across various medical domains, all in a way that keeps you interested and engaged.
More FAQs by IJCP Editorial Team








Recent FAQs


Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article