
 IJCP Editorial Team
IJCP Editorial Team
Ovarian Torsion Premenarch
An
11-year-old girl presented with a two-day history of intermittent left lower
abdomen pain and dysuria, followed by non-projectile vomiting for one
day.
The
child’s parents reported that she had been generally healthy before this
episode. Her past medical history included a similar complaint six months ago,
managed conservatively, and a history of febrile seizures at two years of age.
Her last vaccination was administered at five years of age.
The
initial diagnosis was acute gastroenteritis, which was conservatively managed.
However, her symptoms worsened, leading to severe abdominal pain. Her axillary
temperature was 98.4◦F; pulse rate was 100 per minute; blood pressure was
110/70 mmHg; respiratory rate was 18 breaths per minute; and she had 100%
oxygen saturation on room air. Physical examination revealed absent secondary
sexual characteristics, scaphoid abdomen with normal bowel sounds, tenderness
in the lower abdomen, more severe in the left iliac fossa, involuntary guarding
and rigidity, and absence of rebound tenderness. Systemic examination was
unremarkable, except for the patient’s height (128 cm) and weight (25 kgs),
below the 3rd percentile for her age.
Laboratory
results showed an elevated white blood count, while her hemoglobin, hematocrit,
and platelets were within normal levels.
Temporary
relief from pain and vomiting was achieved with intravenous analgesics and
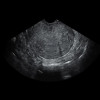
antiemetics. Ultrasonography with Doppler study revealed a heterogeneous mass
in the left adnexal region, suggesting left-sided adnexal torsion. MRI of the
pelvis confirmed the diagnosis, showing an enlarged left ovary with twisting of
the vascular pedicle. Emergency laparoscopy revealed an enlarged left ovary with
a hemorrhagic cyst, diagnosed as ovarian torsion.
Detorsion,
aspiration of the cyst, and bilateral oophoropexy were performed. The patient
was discharged in stable condition, and follow-up ultrasounds demonstrated a
reduced size of the left ovary and normal right ovary, emphasizing the
significance of prompt diagnosis and management of ovarian torsion in pediatric
patients.
Using ultrasound as a first-line imaging modality, particularly in resource-poor settings, is crucial. Conservative surgical intervention with ovarian sparing surgery and oophoropexy are the most effective treatment modalities––preventing recurrences and achieving positive outcomes.
Source: Wani F J,
Nagendhar Y, Reddy R. Indian J Obstet Gynecol Res. 2023;10(4):494-497
IJCP Editorial Team
Comprising seasoned professionals and experts from the medical field, the IJCP editorial team is dedicated to delivering timely and accurate content and thriving to provide attention-grabbing information for the readers. What sets them apart are their diverse expertise, spanning academia, research, and clinical practice, and their dedication to upholding the highest standards of quality and integrity. With a wealth of experience and a commitment to excellence, the IJCP editorial team strives to provide valuable perspectives, the latest trends, and in-depth analyses across various medical domains, all in a way that keeps you interested and engaged.
More FAQs by IJCP Editorial Team






Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article