Pheochromocytoma/Paraganglioma (PPGL) during Pregnancy
A 25-year-old woman who was 31 weeks into her first pregnancy, was hospitalized following a hypertensive episode during a dental procedure. She had been reportedly healthy prior to her pregnancy.
Upon admission, her physical exam revealed high blood pressure (BP) of 150/90 mmHg while supine, a heart rate (HR) of 130 bpm, and no edema in her lower limbs. Her pre-pregnancy body mass index (BMI) was 18 kg/m². Blood tests showed mild anemia, leukocytosis without deviation, and abnormal inflammatory markers.
The provisional diagnosis was preeclampsia. However, her BP became increasingly difficult to control, and hyperglycemia developed.
Further medical history revealed episodes of sweating and palpitations that continued during pregnancy. Suspecting a pheochromocytoma or paraganglioma (PPGL), plasma metanephrines were tested.
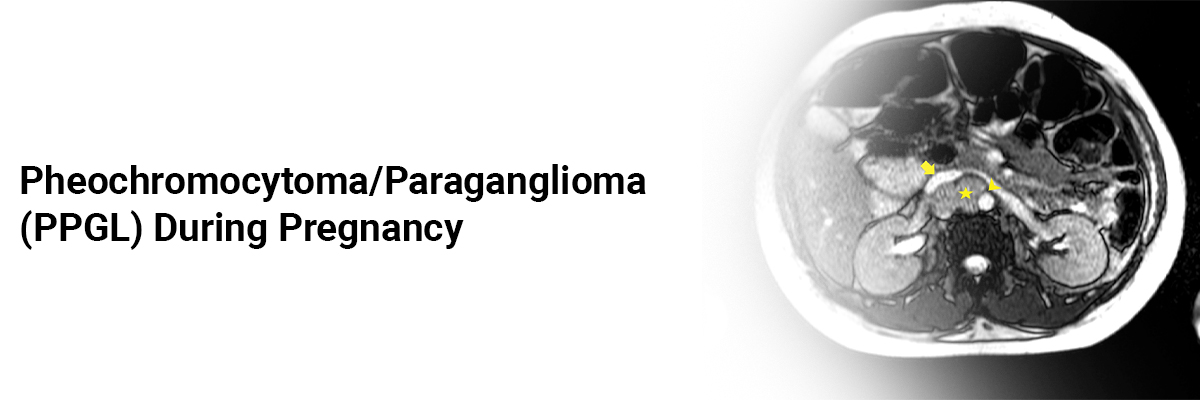
An abdominal MRI identified a 41 × 33 × 42 mm retroperitoneal mass near the right kidney with T2 enhancement, indicative of paraganglioma. Due to persistent labile hypertension, the medical team decided to conduct anemergency cesarean delivery at 32 weekswithout prior adrenergic receptor blockade. During surgery, BP spiked to 260/192 mmHg and HR to 225 bpm.
Post-delivery, the patient required norepinephrine and sodium nitroprusside. She was then started on oral alpha-blockers, which contraindicated breastfeeding. Postoperatively, BP and plasma glucose levels normalized, and outpatient follow-up showed no complications.
The newborn weighed 2,370 grams with Apgar scores of 8 and 9 at 1 and 5 minutes. The placenta weighed 430 grams, showed third-trimester morphology, bleeding, and focal villous necrosis, but no membrane or umbilical cord changes.
One week post-delivery, plasma normetanephrines were ten times the upper limit of normal, and metanephrines were normal. Iodine-131 metaiodobenzylguanidine (131I-MIBG) scintigraphy confirmed PPGL – with significant radioiodine uptake above the right kidney.
A video laparoscopic resection of the mass was performed four months later, following effective adrenergic blockade. Pathological examination revealed a 19 g PPGL (4.0 × 3.4 × 2.6 cm) with a low histological grade.
Despite its rarity, PPGL should be considered in the differential diagnosis of hypertension during pregnancy, especially if it presents early or worsens during gestation. Misdiagnosis and improper treatment can result in severe consequences for both mother and fetus, including fetal hypoxemia, intrauterine growth restriction, prematurity, and fetal death.
PPGLs diagnosed during reproductive years are often due to a genetic predisposition, necessitating genetic investigation and counseling. Early diagnosis of PPGL is crucial for better maternal and fetal outcomes, enabling proper surgical preparation and appropriate delivery decisions to reduce morbidity and mortality. Although a PPGL diagnosis during pregnancy can be distressing, coordinated management by a multidisciplinary team can provide significant relief for the patient and her family.
Source: Giorgi RB, Aroucha PT, Favreto TM, et al. Case Reports in Obstetrics and Gynecology. 2024;2024(1):6655229.

Recent FAQs





Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article