Trachelectomy After Supracervical Hysterectomy: A Case Study
A 55-year-old postmenopausal woman presented to a tertiary care center with a two-year history of a mass protruding per vaginum.
The lady had been menopausal for the last 10 years and had a history of two vaginal deliveries. Her last childbirth was 28 years ago, and she underwent laparoscopic sterilization 26 years ago. Additionally, she had an abdominal hysterectomy for fibroids 10 years back and was diagnosed with hypertension four months prior.
On physical examination, her BMI was 23.4. Abdominal examination revealed a soft, non-tender abdomen with a transverse scar. Pelvic examination showed the cervix at the level of the external OS, a grade three cystocele, and no signs of stress urinary incontinence. A uterine sound could not be passed beyond one centimeter, and the cervix was stenosed without tenderness.
Laboratory investigations, including complete blood count, liver and kidney function tests, were normal. However, glucose levels were elevated with an HbA1c of 10%. Urine analysis showed no ketones, and urine culture was negative. Pap smear was negative for intraepithelial lesions or malignancy. Ultrasound revealed a small cervical stump approximately two centimeters in length.
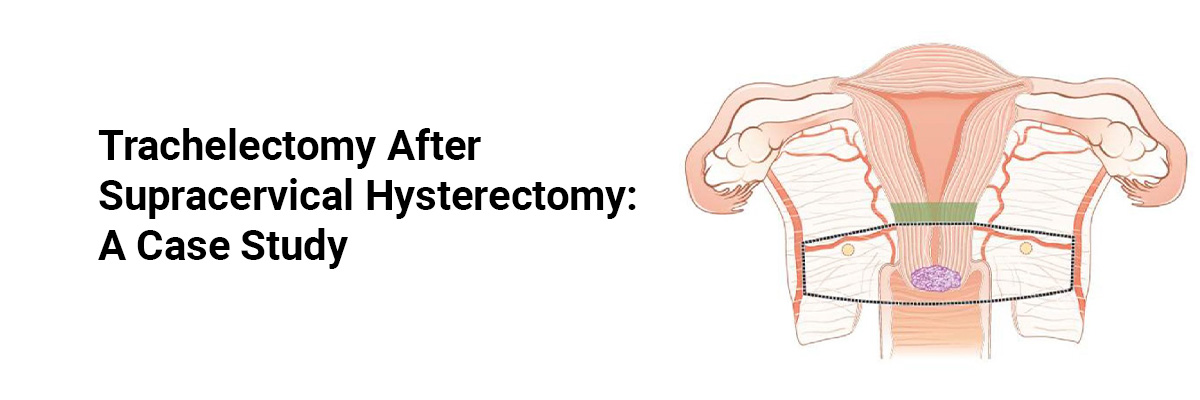
Given her history of supracervical hysterectomy (SCH) and the presence of cervical descent and cystocele, the patient underwent trachelectomy and anterior colporrhaphy. Intraoperatively, a four-centimeter cervical length with grade three cystocele was noted, with no evidence of enterocele. The procedure included careful dissection of the bladder from the cervical stump, identification of the uterosacral ligaments, and removal of the cervical stump, followed by closure of the vaginal mucosa. The histopathological report confirmed chronic cervicitis.
The postoperative period was uneventful, and the Foley catheter was removed after 48 hours. At the six-month follow-up, the patient reported no issues. The vaginal approach to trachelectomy, particularly in cases of retained cervical stump with prolapse, is straightforward and allows for simultaneous pelvic floor repair.
For patients with a retained cervical stump presenting with prolapse after SCH, a simple vaginal trachelectomy with cystocele repair is an effective treatment option.
Source: Ballal P, Pandit MD. Indian Obstetrics and Gynaecology. 2024 Jul 23;14(2).

Recent FAQs





Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article